The scan is not the diagnosis
Seeing “herniated disc” on an MRI report is unsettling, and many patients arrive assuming the operation is already decided. It usually isn’t. A herniation on imaging is an important finding, but it is not the whole diagnosis. I make treatment decisions by matching the scan against your symptoms, your physical exam, your neurologic function, and how things are changing over time.
What a herniated disc actually is
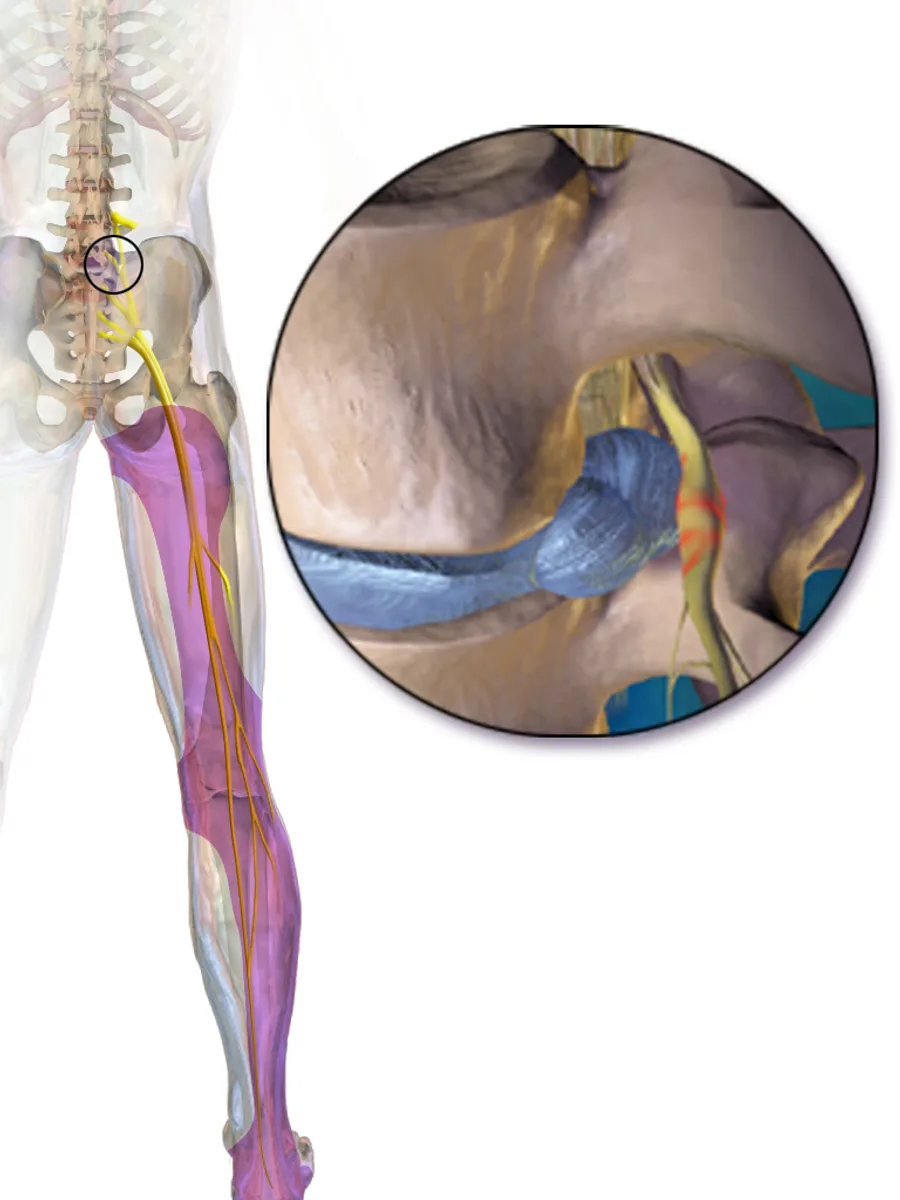
The discs are soft cushions between the bones of the spine. Each one has a tough outer ring and a softer center. A herniation happens when some of that inner material pushes through the outer layer. In the low back, it can press on or inflame a spinal nerve, so the pain travels from the back or buttock down the leg. That is what most people call sciatica, or lumbar radiculopathy.
The key point: a herniation is an imaging finding. It only becomes clinically meaningful when it explains the pain you actually have.
Why the MRI isn’t the whole story
MRI is excellent at showing discs, nerves, and soft tissue. It is also very good at showing things that aren’t causing any pain at all. Disc bulges, degeneration, and even frank herniations turn up routinely in people with no back or leg pain, and they become more common with age. That is why the report should never be read in isolation.
So the useful question isn’t “Do I have a herniated disc?” It is “Does this herniated disc explain my symptoms?” A herniation is far more likely to be the real culprit when:
- The pain travels down a specific nerve pathway, not just a vague ache.
- The scan shows pressure on the same nerve that matches that pattern.
- The exam agrees, with weakness, numbness, reflex changes, or a positive straight-leg raise.
- Leg pain dominates over generalized low-back soreness.
- The symptoms are severe, persistent, or worsening despite good treatment.
When the scan and the symptoms don’t line up, that is a reason to slow down and look harder, not to rush to surgery.

The symptoms that matter most
A truly symptomatic disc herniation usually causes nerve-type pain: sharp, burning, electric, or shooting. The things I pay closest attention to are:
- Pain traveling from the low back or buttock down the leg.
- Numbness or tingling in the leg or foot.
- Weakness in the leg, ankle, or foot.
- Pain that worsens with sitting, coughing, sneezing, or bending.
- Trouble walking normally because of pain or weakness.
The pattern matters as much as the presence of pain. One nerve sends pain down the back of the leg; another sends it into the front of the thigh, the shin, or the top of the foot. Whether the pain follows a recognizable nerve path is a large part of how I judge whether the MRI finding is relevant.
How the diagnosis is actually made
Putting the label on a scan takes three steps, in order.
Your story. I ask where the pain starts, where it travels, what makes it worse, and whether there is numbness or weakness. The path the pain follows is often the most telling part.
The exam. I check strength in the hip, knee, ankle, and foot, along with sensation across the leg and your reflexes. I also watch how you walk, whether you can heel-walk and toe-walk, and nerve-tension signs such as a straight-leg raise.
The imaging. Only then do I read the MRI, looking at whether the herniation compresses the nerve that matches your story and your exam. That correlation is what turns an imaging finding into a diagnosis.
Leg pain and back pain are not the same problem
This is one of the most important points for anyone considering surgery. Disc surgery is most predictable when the main symptom is leg-dominant nerve pain. It is far less predictable when the main symptom is generalized low-back pain.
That doesn’t mean back pain isn’t real. It means its source is more complex. Muscles, joints, ligaments, arthritis, posture, inflammation, and deconditioning can all play a part. A microdiscectomy is designed to remove disc material pressing on a nerve and relieve the sciatica. It is not designed to make every abnormality on a scan look normal.
When a herniated disc improves without surgery
For most people the first move is not the operating room. The body calms the inflammation around the nerve, and the herniated material often shrinks or is reabsorbed over weeks to months. Symptoms settle even when the scan still looks dramatic.
Non-surgical care is not “doing nothing.” It is an active plan, which may include:
- Modifying activity while staying mobile.
- Avoiding prolonged bed rest.
- Anti-inflammatory medication when appropriate.
- Physical therapy or guided exercise.
- Walking and gradual conditioning.
- A targeted epidural steroid injection in selected cases.
- Time for the nerve inflammation to settle.
The goal is to reduce pain, protect function, and let the condition declare itself. A large share of patients never need surgery, and those who recover this way do just as well long term as those who operate early. If symptoms are steadily improving, surgery may not be necessary even when the MRI still looks abnormal. Choosing not to operate is a real treatment, not a delay.
When surgery may be considered
Surgery becomes the better option when the diagnosis is clear and the symptoms stay disabling despite a fair trial of non-surgical care. You are more likely to be a good candidate when:
- Leg pain is the dominant symptom.
- The pain follows a clear nerve pattern.
- The MRI shows compression of that same nerve.
- Symptoms haven’t improved with non-surgical care.
- Pain interferes with sleep, work, walking, or daily life.
- Weakness is present or worsening.
- You understand the goals, limits, and risks of the operation.
For most patients this is an elective decision. The aim is faster, more reliable relief of nerve pain, not correcting every age-related change on the scan. A clean target is what makes the result predictable, which is exactly why I would rather wait for a clear picture than operate on an unclear one.
What surgery may involve
For a lumbar herniated disc causing sciatica, the most common operation is a microdiscectomy. I carefully remove the portion of disc material pressing on the nerve. The procedure is usually focused, limited, and done with a minimally invasive approach. Some patients are candidates for endoscopic techniques. The right approach depends on where the herniation sits, your anatomy, your overall health, and surgical judgment.
A fusion is not needed for simple disc herniations. In cases of recurrent disc herniation or advanced degeneration, a disc replacement is sometimes the better option.
What recovery looks like
Recovery varies, but leg pain often eases before numbness or weakness do. Nerve recovery takes time, especially when the nerve was compressed for a long stretch before surgery. Most patients are encouraged to walk early while avoiding heavy bending, lifting, and twisting during the initial healing period. Return to work depends on your job, the procedure, your neurologic status, and how you are healing.
It is worth keeping expectations realistic. Surgery can be very effective for a well-matched nerve compression, but it does not guarantee complete pain relief, prevent every future disc problem, or eliminate all back pain.
Don’t wait on these
Most herniations leave time for a careful decision. A handful of symptoms don’t. Get evaluated promptly, and the same day for anything involving the bladder, bowel, or saddle area, if you notice:
- New or worsening weakness in the leg.
- Trouble lifting the foot, or tripping repeatedly.
- Loss of bladder or bowel control.
- Numbness in the groin or saddle area.
- Progressive numbness or difficulty walking.
- Severe, unrelenting pain at night.
- Fever together with severe back pain.
- New spine pain after a significant injury, or with a history of cancer.
These don’t always mean surgery is needed, but they should never be ignored.
A few common misconceptions
“The bigger the herniation, the worse the pain.” Not always. A small herniation in the wrong place can irritate a nerve severely, while a large one may cause few symptoms if it isn’t pressing on anything sensitive.
“An abnormal MRI means surgery is inevitable.” No. Many abnormalities improve, or stop hurting, without an operation.
“If I wait, I’ll permanently damage the nerve.” Usually not, as long as strength is stable and there are no emergency symptoms. Worsening weakness or bladder and bowel changes are what shift the timeline.
“Surgery fixes the whole disc.” A discectomy removes the fragment pressing on the nerve. It doesn’t replace the disc or reverse degeneration.
“If the pain comes from a disc, physical therapy can’t help.” Therapy won’t push the disc back. But it can ease symptoms, calm a sensitive nerve, and restore movement.
Questions worth asking before you decide
A good consultation should leave you understanding not just what the MRI shows, but why it does or doesn’t explain your pain. It is fair to ask:
- Which nerve looks compressed, and do my symptoms match it?
- Is my pain mostly nerve pain, back pain, or both?
- Am I improving, stable, or worsening?
- What non-surgical options are still reasonable?
- If you would recommend surgery, what exactly is the goal, and would it help my leg pain, back pain, or both?
- What are the risks of waiting versus operating, and what would make surgery more urgent?
If you have a herniation on the scan, real pain, and no clear answer about what to do next, that’s exactly what a consultation is for. A second opinion exists for precisely this.
Common questions
Does a herniated disc on an MRI always cause pain?
No. Many people have disc bulges, degeneration, or herniations on an MRI without any symptoms. A herniation matters most when it matches the pain pattern and the exam findings.
Can sciatica from a herniated disc improve without surgery?
Often, yes. Many patients improve over weeks to months with non-surgical care, especially when weakness is absent or stable and symptoms are trending in the right direction.
How long should I wait before considering surgery?
There is no single timeline. Many patients try non-surgical care first if neurologic function is stable. Surgery may be discussed sooner when pain is severe, function is poor, or weakness is present.
Can a disc herniation come back after surgery?
It can. Recurrent herniation is possible, and the risk depends on patient-specific factors such as disc anatomy, activity level, smoking status, and body mechanics.
Do I need a fusion for a herniated disc?
Rarely, if ever. A minimally invasive microdiscectomy is the answer initially. Recurrent herniations may require a disc replacement or fusion. We can discuss this further during our consultation.
When is a herniated disc an emergency?
Loss of bladder or bowel control, numbness in the saddle area, or rapidly worsening weakness needs urgent medical evaluation the same day.
This article is for general educational purposes and is not medical advice. It does not create a doctor–patient relationship. For guidance about your own spine, see a qualified physician.